The 80% Problem: Why Most Medical Bills Are Wrong

Executive Summary: Industry analyses report 49-80% of medical bills contain at least one error. Common mistakes include duplicate charges, upcoding, NCCI bundling violations, and pharmacy markups reaching 500-10,000% over acquisition cost. For practices, billing errors erode patient trust and trigger online reviews blaming you for errors you didn’t create. For patients, the errors often total hundreds to thousands of dollars per visit. The fix: request itemized statements, cross-reference against EOBs, and use automated analysis to catch technical violations.
Sarah paid $4,200 for her son’s ER visit. Three months later, she found $1,800 in errors—duplicate charges for the same blood draw, a medication he’d refused, and a Level 5 visit code for what was actually a Level 3.
She got a refund. But first, she left a one-star Google review.
Dr. Patel’s urgent care didn’t make those errors. The hospital did. But Sarah’s review didn’t mention that. It just said “billing nightmare” and named the facility.
This is the part nobody talks about: billing errors don’t just cost patients money. They cost practices trust.
The Scope of the Problem
Medical billing errors aren’t occasional glitches. Industry analyses report that 49-80% of medical bills contain at least one mistake, a range based on studies from medical billing auditors and healthcare researchers. The variability reflects different methodologies and bill types, but the direction is consistent: errors are common.
The financial stakes are significant:
-
For patients: Billing errors on hospital bills frequently total hundreds to thousands of dollars per visit. The Kaiser Family Foundation reports that Americans collectively hold over $220 billion in medical debt, with billing inaccuracies contributing to balances that should never have existed.
-
For practices: Each denied claim costs $25-30 to rework. A single upcoding pattern flagged by a payer can trigger a full audit. And patient disputes over billing—even when the error originated elsewhere in the care chain—damage online reputation and referral relationships.
The system isn’t broken because anyone is acting in bad faith. It’s broken because it’s absurdly complex.
Why Billing Errors Are Systemic, Not Exceptional
A single emergency department visit can generate separate charges from the hospital facility, the attending physician, the radiologist reading the scan, the laboratory processing bloodwork, and an anesthesiologist who may be employed by a third-party staffing company. Each entity bills independently, often using different software, different coding staff, and different claim submission timelines.
The coding infrastructure compounds the challenge. Medical billers select from over 10,000 CPT procedure codes and 70,000+ ICD-10 diagnosis codes. A billing specialist processing dozens of patients per hour can easily select an adjacent code from a dropdown menu—charging for a complex visit when the documentation supported a moderate one.
Then there’s payer complexity. When claims are denied or partially paid, the remaining balance sometimes lands on the patient even when it shouldn’t. Coordination of benefits between multiple policies (employer coverage plus Medicare, for example) creates gaps where charges fall through. The No Surprises Act added critical protections starting in 2022, but enforcement is uneven and billing departments don’t always apply the rules correctly.
For clinicians, these aren’t abstract problems. They show up as:
- Phone calls from confused patients who don’t understand why they owe $800
- Online reviews blaming your practice for a billing error you didn’t create
- Staff hours burned on billing disputes instead of patient care
- Compliance exposure from coding patterns you didn’t know existed
Tools like ORBDOC’s Medical Bill Analyzer exist precisely because this complexity exceeds what any individual—patient or practice—can reasonably track manually. The technology scans bills against Medicare pricing files, NADAC drug acquisition costs, NCCI bundling rules, and known error patterns. For patients, it’s self-defense. For practices, it’s a resource to hand patients before they leave a frustrated voicemail.
Example: A Real Hospital Itemized Bill
This is what complexity looks like in practice:
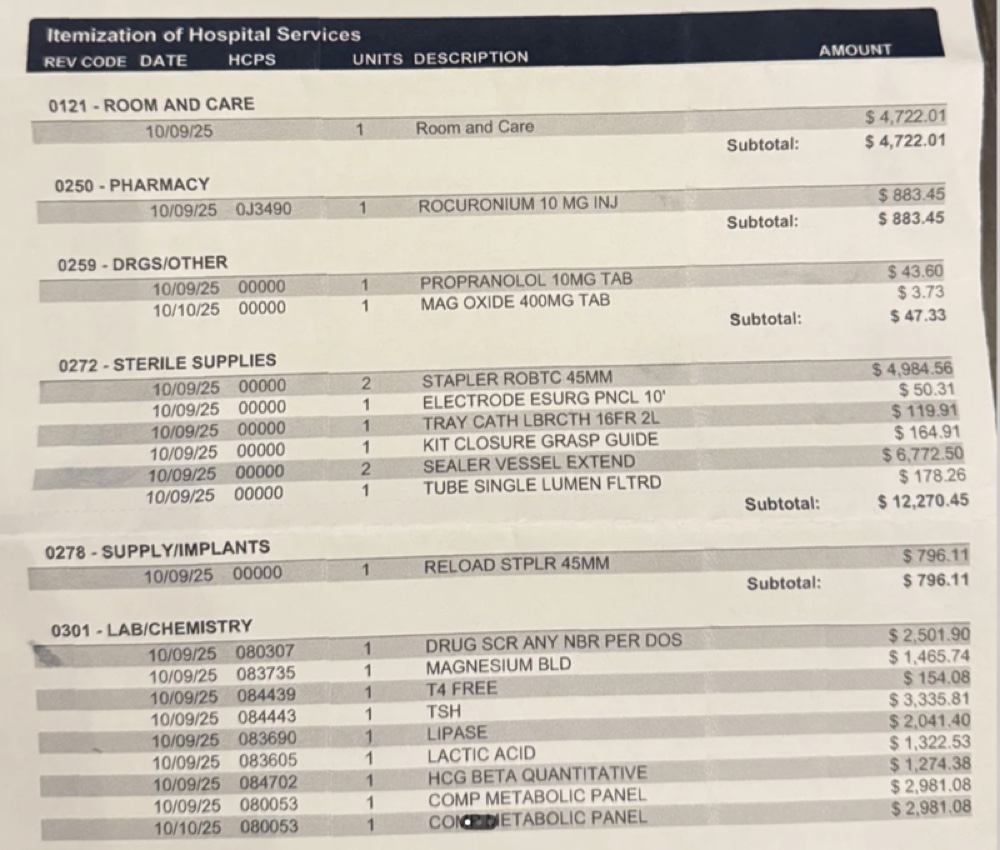 A typical hospital itemized statement with hundreds of line items across multiple departments—room charges, pharmacy, laboratory, and medical supplies. Each line item represents a potential error point.
A typical hospital itemized statement with hundreds of line items across multiple departments—room charges, pharmacy, laboratory, and medical supplies. Each line item represents a potential error point.
What to look for:
- Duplicate charges: Same CPT code appearing multiple times on the same date
- Department crossover: Did pharmacy and nursing both charge for the same medication?
- Quantity verification: Does the billed quantity match what was actually administered?
- Description accuracy: Do the procedure codes match the plain-language descriptions?
Complex hospital bills often contain multiple errors that total hundreds or thousands of dollars in overcharges. Manual review requires cross-referencing dozens of codes against multiple databases. Automated analysis streamlines this process significantly.
Common Error Patterns That Appear on Medical Bills
Whether you’re a patient auditing your own statement or a practice manager reviewing claims, the same patterns recur.
1. Duplicate Charges
The same service billed twice. This happens when different departments independently log the same procedure, when EHR systems glitch during claim submission, or when manual entry errors go unreviewed. Look for identical line items with matching dates.
How ORBDOC Detects It: The Bill Analyzer flags any CPT or HCPCS code that appears more than once, calculating the potential overcharge amount for review.
2. Upcoding
Billing for a higher-complexity service than what was provided. A routine office visit coded as comprehensive. Generic medication charged at brand-name rates. Upcoding is sometimes intentional fraud, but more often, it’s a coding error that nobody caught.
For clinicians: Upcoding patterns in your claims data, even if unintentional, can trigger payer audits and recoupment demands. Proactive review matters.
How ORBDOC Detects It: The analyzer compares charged amounts against Medicare rates. When a charge exceeds 400% of the Medicare reference rate (the “extreme markup” threshold), the system flags it for review with specific dollar amounts and markup percentages.
3. Unbundling (NCCI Bundling Violations)
Procedures that should be billed together at a package rate are instead split into separate line items that cost more when totaled. This is called an “unbundling violation” or “NCCI violation.” CMS publishes detailed bundling rules through the National Correct Coding Initiative (NCCI)—for example, a Comprehensive Metabolic Panel includes specific electrolyte tests that cannot be billed separately.
How ORBDOC Detects It: The Bill Analyzer cross-references submitted codes against NCCI bundling tables for lab panels, surgical repairs, and E/M services. When a parent panel code and its component codes both appear on the same bill, the system identifies the unbundling violation and calculates the overcharge.
4. Balance Billing Violations
The No Surprises Act (effective January 2022) prohibits most surprise out-of-network bills for emergency services and certain non-emergency situations. But billing departments don’t always apply the protection correctly. If a patient received emergency care and faces unexpected out-of-network charges from a provider they didn’t choose, federal law likely applies.
For clinicians: If your practice includes any out-of-network scenarios, your billing team needs explicit NSA compliance protocols. Patient complaints in this area can escalate to regulatory action.
Manual Review Required: This violation type typically requires reviewing insurance contracts and provider network status—factors that automated systems can’t always access.
5. Pharmacy Markup Violations (Hospital Drug Overcharges)
Hospital pharmacy charges can exceed acquisition costs by 500-10,000%. This is one of the most common and expensive billing errors. The Bill Analyzer detects these pharmacy markups using three data sources:
-
Curated J-Code Pricing: For common injectable drugs (chemotherapy, biologics, vaccines), the system uses pharmacy acquisition cost data aligned to HCPCS billing units. When charges significantly exceed acquisition costs (for example, a hospital charging $12,000 for a drug with a $400 acquisition cost), the system triggers a critical-severity alert.
-
NADAC Lookup: For NDC-coded medications, the system references the National Average Drug Acquisition Cost database—the price pharmacies actually pay wholesalers.
-
Medicare ASP: For drugs without curated or NADAC data, the system uses Medicare’s Average Sales Price as a baseline, flagging charges exceeding 8x the ASP rate.
How ORBDOC Detects It: When a line item contains a J-code (e.g., J1745 for Remicade) or NDC code, the analyzer calculates the markup percentage against acquisition cost and flags violations exceeding 500%. The severity escalates from “warning” (5x markup) to “critical” (100x+ markup).
Real Example: Pharmacy Markup Detection
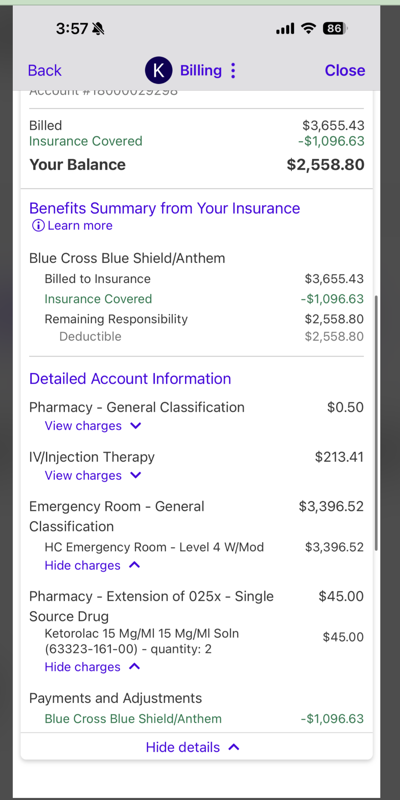 Emergency room bill showing drug charges using J-codes (HCPCS codes starting with “J”). The Bill Analyzer cross-references these against NADAC acquisition costs and Medicare ASP rates.
Emergency room bill showing drug charges using J-codes (HCPCS codes starting with “J”). The Bill Analyzer cross-references these against NADAC acquisition costs and Medicare ASP rates.
What the analyzer checks:
- J-code identification: Is this a drug code (J0000-J9999)?
- Acquisition cost lookup: What does the hospital pay wholesalers for this drug?
- Markup calculation: Is the patient charge 5x, 10x, or even 100x the acquisition cost?
- Reasonable hospital charge: Flags charges exceeding 500% of acquisition cost
For this specific bill, the analyzer would flag any J-code charges exceeding 5x the NADAC acquisition cost with severity levels based on markup magnitude. A 10,000% markup (100x cost) triggers a critical alert.
6. Drug Quantity and Unit Verification
Many billing errors occur because J-codes are priced per specific units (e.g., per 10mg), but hospitals sometimes bill incorrectly by vial quantity or total milligrams. The system alerts patients to verify that billed quantities align with what was actually administered.
How ORBDOC Detects It: Cross-references billed drug codes and quantities against standard HCPCS dosage definitions, prompting patients to verify the quantity matches their medical records.
7. Good Faith Estimate Violations
Under the No Surprises Act, uninsured and self-pay patients must receive cost estimates before scheduled services. Bills exceeding the estimate by $400+ can be disputed through a federal process.
How ORBDOC Detects It: When users input both an estimate amount and final bill amount, the analyzer calculates the discrepancy and identifies when it crosses the $400 threshold that triggers federal dispute rights.
8. Services Never Rendered
Charges for procedures that were discussed but canceled. Medications the patient declined. Lab work accidentally attributed from another patient’s account. These errors are often the easiest to dispute—but only if someone actually reviews the itemized bill against what happened.
Manual Review Required: Requires patient or provider recollection of what actually occurred during the visit.
9. Incorrect Patient Information
A misspelled name, outdated insurance ID, or wrong date of birth can cause an entire claim to be denied—leaving the patient facing full charges. Simple to fix once identified, but frequently overlooked.
Manual Review Required: Check demographic information against insurance card and records.
For Patients: How to Audit Your Medical Bill in 30 Minutes
You don’t need medical training to audit your medical bill. You need an itemized bill and a systematic approach.
Step-by-Step Bill Analysis Example
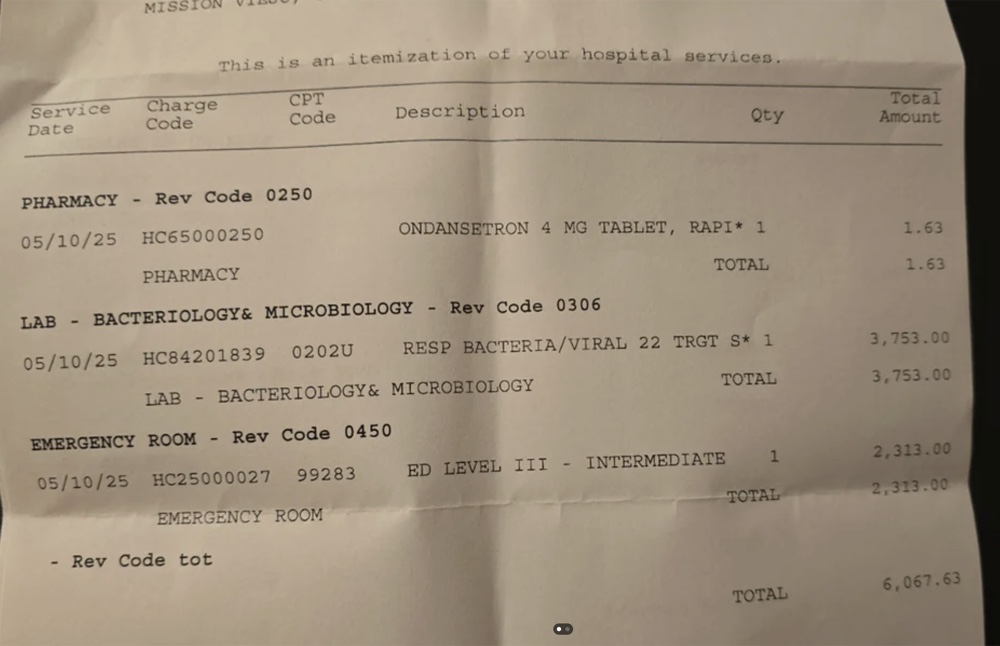 An ER itemized bill showing the level of detail needed for effective auditing. Notice the CPT codes (99283 for ER visit), pharmacy charges, and lab work—each requires verification.
An ER itemized bill showing the level of detail needed for effective auditing. Notice the CPT codes (99283 for ER visit), pharmacy charges, and lab work—each requires verification.
What this bill reveals:
- CPT 99283: Emergency visit code (Level 3) - Verify this matches visit complexity
- Pharmacy line items: Each drug should have quantity, NDC or J-code, and per-unit pricing
- Lab charges: Check for bundling violations if multiple lab panels appear
- Duplicate check: Scan for identical codes with the same date of service
Step 1: Request the itemized statement. Summary bills only show totals—useless for identifying errors. Call the billing department and request the line-by-line version with dates, procedure codes, and individual charges. You have a legal right to this document.
Step 2: Compare against your Explanation of Benefits. Your insurer’s EOB shows what was billed, what they paid, and what you owe. Discrepancies between the EOB and the provider’s bill indicate errors. Don’t pay until they match.
Step 3: Cross-reference your memory. Did you actually receive every service listed? Do the dates align? Were any procedures canceled or modified? Your recollection is evidence.
Step 4: Use automated analysis. Upload your bill to ORBDOC’s Bill Analyzer to automatically decode CPT codes, flag duplicates, detect NCCI bundling violations, identify extreme markups against Medicare rates, and calculate pharmacy overcharges using NADAC acquisition data. This significantly reduces the time needed for comprehensive bill review.
Step 5: Check pricing benchmarks. Healthcare Bluebook and FAIR Health Consumer show typical costs by procedure and geography. Significant outliers warrant questions—not accusations, but questions.
Step 6: Verify the math. Add the itemized charges yourself. Confirm that insurance payments were credited. Sometimes the totals are simply wrong.
For Clinicians: Why Billing Accuracy Is a Practice Management Issue
Most clinical leaders think of billing errors as a patient problem. It’s not. It’s a practice problem with downstream effects on:
Patient trust. A patient who receives a confusing or inaccurate bill doesn’t distinguish between your care and your billing. They remember frustration. They tell friends. They leave reviews.
Staff efficiency. Every billing dispute that escalates to your front desk is 15-30 minutes of staff time. Multiply by volume. That’s hours per week spent on defensive conversations instead of patient care.
Compliance exposure. Upcoding and unbundling patterns—even unintentional ones—can trigger payer audits. Recoupment demands. In extreme cases, fraud investigations. “We didn’t know” is not a defense.
Revenue cycle integrity. Denied claims cost $25-30 each to rework. Patterns of denial indicate systematic coding issues. Catching them early protects cash flow.
What high-performing practices do differently:
-
Audit a sample of claims monthly. Even 5-10% review catches patterns before they become audit triggers. Use the Medical Billing Code Atlas to understand denial risks by procedure.
-
Give patients a resource before they call angry. Pointing patients toward a tool like ORBDOC’s Bill Analyzer—proactively, at discharge—signals that you care about their financial experience. It also deflects billing questions to a system designed to answer them.
-
Train front desk staff on common billing questions. Most patient frustration comes from feeling unheard. A staff member who can explain “here’s how to read your EOB” de-escalates faster than one who says “you’ll have to call billing.”
-
Track billing-related complaints as a quality metric. If billing complaints are rising, something in the revenue cycle is broken. Treat it like you’d treat a clinical quality signal.
The Regulatory Landscape Is Shifting
Several recent policy changes make billing accuracy more urgent—and more enforceable:
No Surprises Act (2022): Prohibits most surprise out-of-network bills for emergency services. Establishes an independent dispute resolution process. Enforcement is ramping up.
Hospital Price Transparency Rule (2021, expanded 2024): Requires hospitals to publish machine-readable pricing files. Patients can now comparison shop—and identify outlier charges.
Medical Debt and Credit Reporting (2023): Major credit bureaus removed most medical debt under $500 and extended reporting delays. This reduces some patient harm, but doesn’t fix the underlying billing errors.
Good Faith Estimate Requirements: Uninsured and self-pay patients must receive cost estimates before scheduled services. Bills exceeding the estimate by $400+ can be disputed through a federal process.
For patients, these rules provide new leverage. For practices, they raise the stakes on billing accuracy and transparency.
What to Do Right Now
If you’re a patient:
Pull the last medical bill you paid—or the one sitting on your counter. Request the itemized version if you don’t have it. Upload it to ORBDOC’s Medical Bill Analyzer and let the system flag duplicates, NCCI violations, extreme markups, and pharmacy overcharges automatically.
You might find nothing. But with error rates this high, odds are you’ll find something.
If you’re a clinician or practice administrator:
Ask your billing team three questions this week:
- What’s our denial rate, and what are the top denial reasons?
- When was the last time we audited a sample of claims for coding accuracy?
- What do we tell patients who call with billing questions—and is that answer good enough?
Then consider what resource you could offer patients proactively. A billing FAQ. A link to price transparency tools. Or a recommendation for ORBDOC’s analyzer as a third-party resource that takes the burden off your staff and demonstrates that you’re on the patient’s side.
The Bottom Line
Sarah got her $1,800 back because she looked. Most patients don’t look. Most practices don’t make it easy.
High error rates in medical billing reflect a system design flaw, not individual negligence. Patients bear the financial cost. Practices bear the reputational cost. And the complexity ensures that nobody catches mistakes unless somebody actively tries.
That’s changing. Price transparency rules are forcing visibility. The No Surprises Act is adding enforcement. And technology is making bill review accessible to anyone with a smartphone—or any practice willing to hand patients a better resource than “call billing.”
The question isn’t whether medical billing is broken. It is.
The question is whether you’re going to keep paying for mistakes—or start catching them.
Frequently Asked Questions About Medical Bill Errors
How can I check my medical bill for errors for free?
Use ORBDOC’s free Medical Bill Analyzer to automatically check for duplicate charges, NCCI bundling violations, pharmacy markups, and extreme pricing against Medicare rates. The tool runs entirely in your browser and doesn’t store or collect your medical data. Simply enter your CPT codes or upload your bill, and the analyzer cross-references charges against Medicare pricing files, NADAC drug acquisition costs, and NCCI bundling rules.
What percentage of medical bills contain errors?
Industry studies report that 49-80% of medical bills contain at least one error. The range varies based on methodology and bill complexity, but research from medical billing auditors, healthcare advocacy groups, and academic studies consistently shows that billing errors are common rather than exceptional. Common errors include duplicate charges, upcoding, unbundling violations, and pharmacy markups.
What is an NCCI bundling violation?
An NCCI bundling violation (also called “unbundling”) occurs when a hospital or provider bills separately for procedures that should be billed together under one code according to CMS’s National Correct Coding Initiative guidelines. For example, a Comprehensive Metabolic Panel (CPT 80053) includes specific electrolyte tests that cannot be billed separately. When both the panel and individual tests appear on the same bill, it’s an unbundling violation that inflates costs.
How do I know if my hospital pharmacy charges are too high?
Compare your pharmacy charges to acquisition costs using NADAC (National Average Drug Acquisition Cost) data—the price pharmacies actually pay wholesalers. Hospital markups of 200-300% over acquisition cost are typical, but markups exceeding 500% indicate potential overcharges. For injectable drugs (J-codes like J1745), hospitals should charge 3-5x the acquisition cost at most. Markups of 1,000-10,000% (10x-100x cost) are billing errors worth disputing.
What should I do if I find an error on my medical bill?
First, request an itemized bill showing all CPT codes, quantities, and individual charges. Compare this against your Explanation of Benefits (EOB) from your insurance company. Document the specific errors you’ve found (duplicate codes, unbundling violations, services not rendered). Contact the billing department in writing, referencing specific line items and CPT codes. Use a free bill checker to identify technical violations like NCCI bundling errors that billing departments are legally required to correct.
Can I dispute a medical bill after I’ve already paid it?
Yes. Most billing departments will review paid bills if you provide documentation of errors within 1-2 years. Keep all itemized bills, EOBs, and payment records. If you identify duplicate charges, unbundling violations, or pharmacy markups after payment, submit a formal dispute letter with specific CPT codes and overcharge amounts. Many patients recover hundreds to thousands of dollars by auditing bills they’ve already paid.
What are the most common medical billing errors?
The six most common billing errors are:
- Duplicate billing - Same CPT code charged multiple times for single service
- Upcoding - Billing for higher-complexity service than provided (e.g., Level 5 visit when documentation supports Level 3)
- Unbundling (NCCI violations) - Billing components separately when they should be bundled
- Pharmacy markups - Hospital drug charges 500-10,000% over acquisition cost
- Services never rendered - Charges for canceled procedures or medications patient declined
- Incorrect patient information - Wrong insurance ID causing claim denials
How long does it take to audit a medical bill?
Manual bill auditing typically requires 30-60 minutes for a simple office visit bill and 2-4 hours for complex hospital bills with hundreds of line items. Using an automated medical bill checker reduces this to 2-5 minutes. The analyzer automatically flags duplicates, NCCI violations, extreme markups, and pharmacy overcharges without requiring manual CPT code lookups or Medicare rate comparisons.
What is NADAC and why does it matter for medical bills?
NADAC (National Average Drug Acquisition Cost) is a database published by CMS showing the average prices pharmacies pay wholesalers for prescription medications. This represents the hospital’s actual acquisition cost before markup. When reviewing pharmacy charges on your medical bill, NADAC pricing reveals whether a hospital’s markup is reasonable (3-5x cost) or excessive (10-100x cost). NADAC data is especially useful for detecting overcharges on generic medications and common injectable drugs.
Should I hire a medical billing advocate?
For bills under $5,000 with obvious errors (duplicates, services not rendered), you can likely dispute them yourself using a free bill analyzer and following the hospital’s dispute process. For bills exceeding $10,000 with complex NCCI violations, pharmacy markup issues, or denied insurance claims, a professional medical billing advocate may be worth the 20-35% contingency fee. Advocates have direct relationships with billing departments and understand payer-specific rules that accelerate dispute resolution.
For Patients: Try ORBDOC’s Medical Bill Analyzer →
For Practices: See How Bill Analysis Reduces Call Volume →
Related Reading
How to Check Your Medical Bill for Errors
Step-by-step guide to finding billing errors, comparing charges to Medicare rates, and knowing when to dispute. Free tool included.
Top 10 Medical Billing Denial Codes in 2025
Which CPT codes get denied most often in 2025 and how to prevent costly claim denials. Research-based denial intelligence for E&M codes.
Finding and Disputing Duplicate Medical Bill Charges
Duplicate billing is one of the most common hospital errors. Learn how to spot the same procedure charged twice and successfully dispute it for a correction.
Understanding the Codes on Your Medical Bill
CPT, HCPCS, revenue codes, modifiers—your medical bill is full of numbers and letters. Here's what they mean and how to use them to spot billing errors.
Next Step
Continue from this guide with practical tools or a product workflow fit check.